At the time that this post is being written, 2.4 million individuals have died from COVID-19, with another 109 million currently infected due to a lack of effective curative or fully preventative measures.
After battling the chaos of mask-wearing, hand-sanitizing, and staying 6 feet apart from one another for the last year, we have now been presented with the advent of a vaccine. Now, we must continue to uphold these measures while facing the challenges of strategic, equitable, and privacy-preserved ways for last-mile vaccine distribution.
In order to achieve such distribution, vaccine recipients must be prioritized to ensure an equitable reach, especially as multiple vaccines with different protocols are approved in various areas. Once an individual’s first dose is administered, they must follow through with their second dose as well.
Currently, paper-based vaccination cards are being used as a way to keep track of COVID-19 vaccinations. Vaccination clinics will also be reporting to their state immunization registries what vaccine was given so that a query could be run if a patient is unsure of when they received their first dose. Every dose administered is also reported to the CDC.
Currently, multiple technological systems are being used by the CDC to combat the challenges that come with this process. The CDC’s Vaccine Administration Management System (VAMS) is a web application that streamlines the vaccine distribution process for jurisdictions, employers, and healthcare providers while allowing users to schedule appointments, receive records of their visit, and receive reminders for a second dose. Their Immunization Information Systems (IIS) is a group of privacy-preserving database systems that track all vaccinations within various areas and their Vaccine Adverse Event Reporting System (VAERS) is the prominent system for the monitoring of health outcomes.
But what if we could do something similar, without wholly eradicating the concept of paper-based vaccination cards? What if we could create a user-centric protocol to augment paper-based vaccination cards instead?

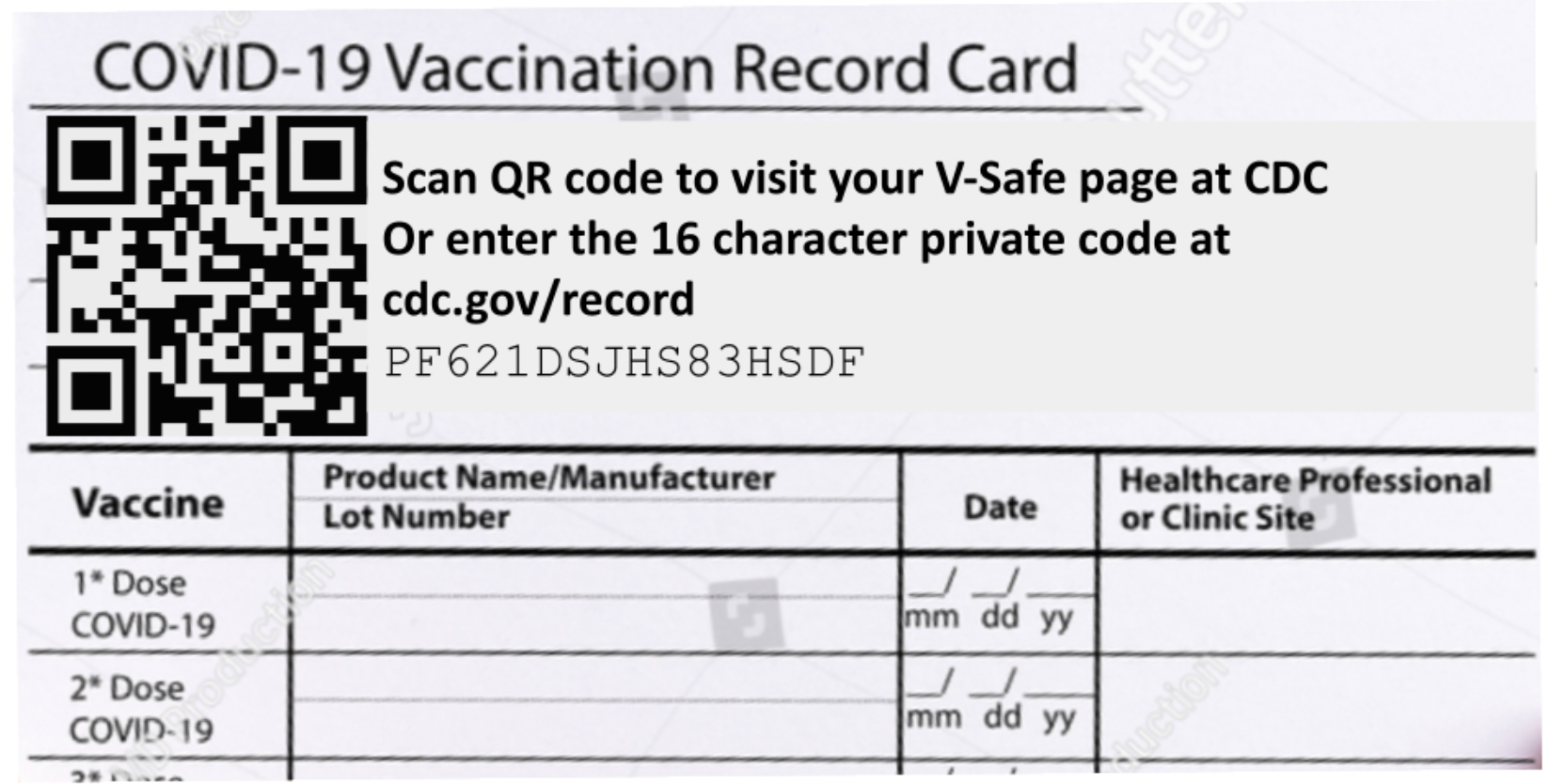
This is exactly what the MIT SafePaths Card (MiSaCa) proposes; augmenting paper-based vaccination cards with printed codes.
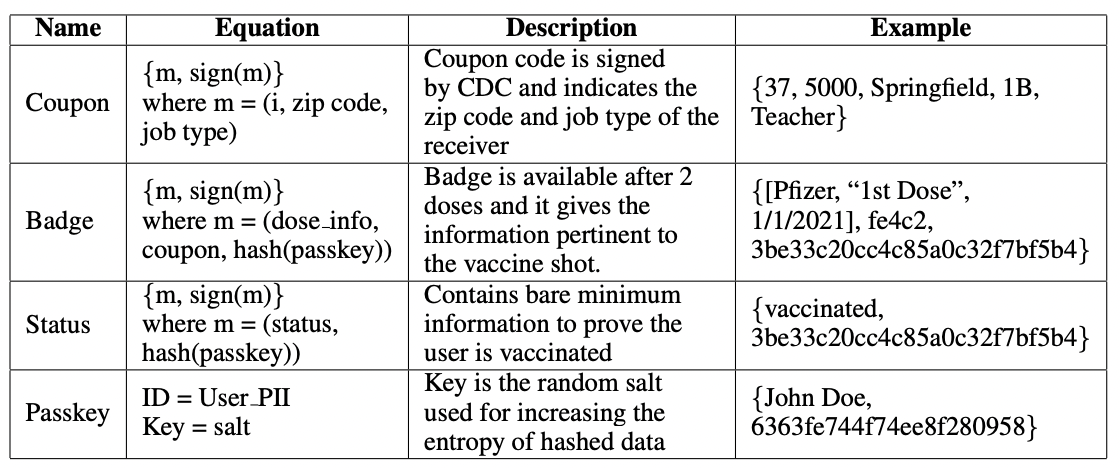
Through this vaccine distribution system, physical SafePaths cards will have four digitally signed QR code stickers, called the Coupon, Badge, Passkey, and Status. The Passkey is the only sticker that contains personally identifiable information (and individual’s name and date of birth). The Coupon gives information about the individual’s city, age, and job; the Badge gives information about the coupon and the dosage info, and the Status reveals if the individual has been vaccinated 0, 1, or 2 times.
Through a QR code system, health information and personally identifiable information is decoupled, essentially separating the eligibility of the vaccine from the distribution of it. This way, the individual’s health information is centralized, while the personally identifiable information is decentralized. Moreover, this streamlined system doesn’t require internet access, as VAMS and VAERS do.
To start, SafePaths cards will be distributed, containing one digitally signed Coupon QR code, provided by a central government agency such as the CDC and made available to users by an employer or local government location.
Check-in at a vaccination clinic would require the verification of a user’s Coupon, and upon vaccination, the clinic would create a digitally-signed record of communication and print it as a QR code on an adhesive sticker, the Badge, containing the time, date, and location of vaccination.
The clinic would also create a unique encryption key for the badge, called the Passkey, containing the individual’s name, age, and sex.
When the user goes to receive a second dose of the vaccine, the clinic would use the user’s Badge to determine to appropriate vaccine type and the Passkey to verify the user’s identity. For further identification, a form of ID can be compared. After the final vaccination, the clinic would create a Status sticker for the user’s SafePaths card indicating that the user has been vaccinated.
Through the method, the user has multiple levels and groups of information they can share, beginning with vaccination status in the unencrypted Status sticker, personal information that must be decrypted using the Passkey sticker, and full personal vaccination information encrypted in the Badge.
Phased vaccination using the SafePaths card system requires the distribution of SafePaths cards with digitally signed Coupons to appropriate subjects during each stage of vaccination. This can be done through dissemination to businesses to provide to employees (g.g. hospitals, restaurants, etc.), making cards available at a local government building, or mailing out to individuals based on employment.
For Coupon verification upon arrival at the clinical, a proposed scanner app would be necessary to scan and verify the digital signature present.
The scanner app would also be able to create digitally signed Badge and Passkey stickers for post-vaccination. It would securely record the vaccine information into a Badge sticker, encrypted using the encryption key present in the Passkey. The second dose administration information would also be implemented in the same manner, and the app would create a Status sticker in a similar manner to the Badge sticker. After creating each of the stickers, the scanner app would not store any information regarding a recipient’s encryption key.
The scanner app would also have the ability to integrate with systems such as VAMS in the united states, and automatically provide vaccination record information. It would also be able to directly aggregate vaccination record data and find population-level statistics which could provide insight for public health policy development.
Using QR codes to augment paper-based vaccination cards can be used for phased vaccine distribution, individual vaccination, second-dose adherence, and symptom follow-up. Due to their nature and simplicity, digitally-signed QR codes may be a convenient mechanism for a larger percentage of the population.
Yet the potential of using QR codes expands far beyond the convenience of vaccination cards. The decentralized storage of the information extends to privacy-focused protocols to low-resource areas and populations, reducing disparities in access to other frameworks of COVID-19 vaccination.
About the PathCheck Foundation
PathCheck Foundation, a generously funded 501(c)(3) non-profit spin-off from MIT, is developing decentralized pandemic response solutions using an open-source, open standard interoperable model. PathCheck is committed to sustained innovation in the middle of rapidly changing protocols, APIs, and epidemiological research in the pandemic response. Previously, PathCheck has delivered Google/Apple Exposure Notification-based full-featured apps in 5 US states/territories and multiple nations. The PathCheck Foundation has now developed a new privacy-preserving approach to vaccine rollout and distribution, utilizing a vaccination app and physical cards. Follow updates at https://pathcheck.org/en/blog.
Source
Bae, J., Sukumaran, R., Shankar, S., Srivastava, S., Iyer, R., Mahindra, A., Mirza, Q., Arseni, M., Sharma, A., Agrawal, S., Mukhopadhyay, O., Kang, C., Katiyar, P., Shekhar, A., Hasan, S., Dasgupta, K., Gandhi, D., TV, S., Patwa, P., Singh, I., Singh, A. and Raskar, R., 2021. MIT SafePaths Card (MiSaCa): Augmenting Paper Based Vaccination Cards with Printed Codes. [online] arXiv.org. Available at: <https://arxiv.org/abs/2101.07931> [Accessed 17 February 2021].